Population Health Approach to Complete Colorectal Cancer Screening Framework and Infographic

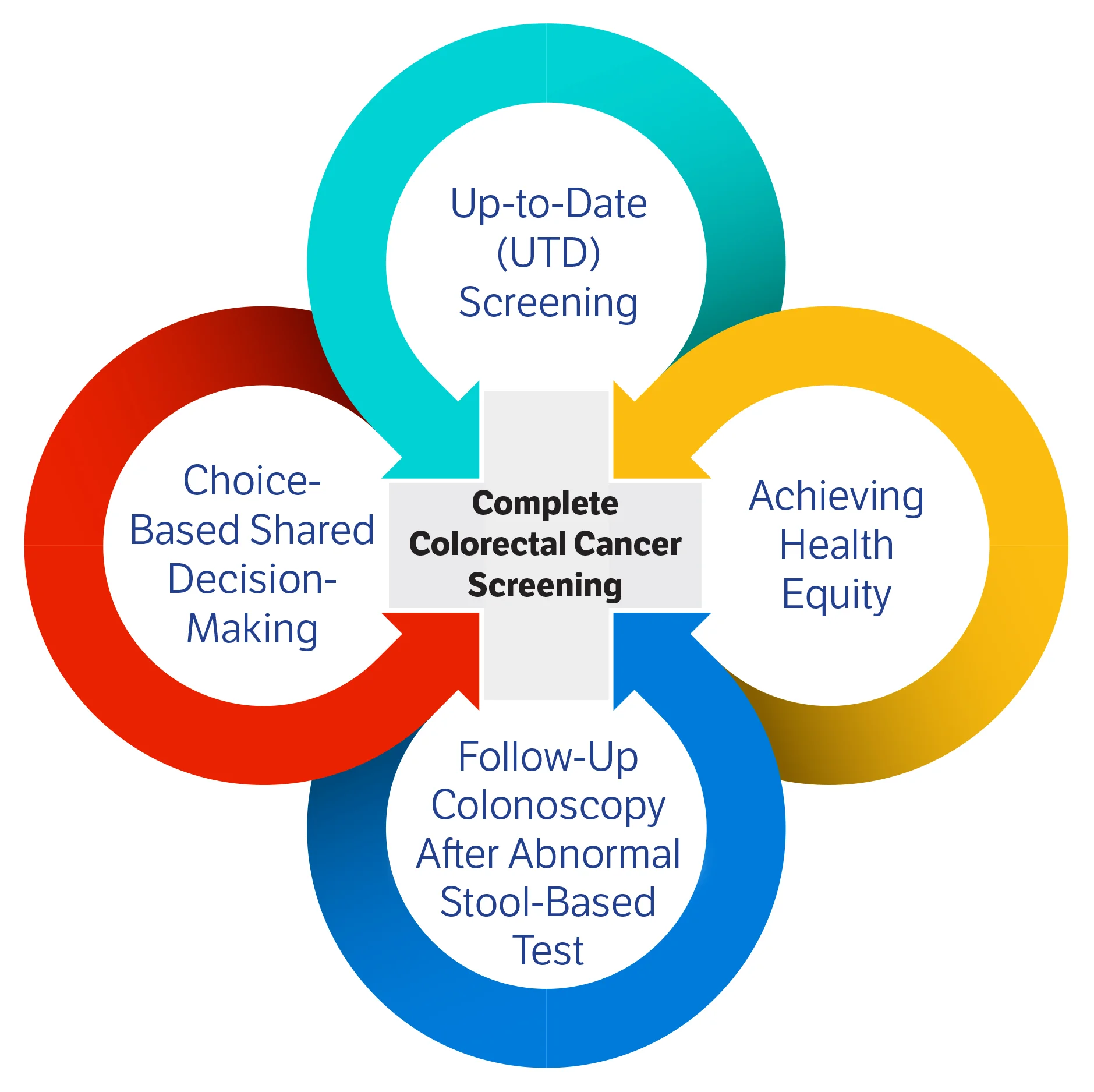
The following colorectal cancer screening components, as seen in the Population Health Approach to Complete Colorectal Cancer Screening Framework, were identified as essential and tested by Collaborative participating healthcare organizations (HCOs).
Implemented interventions with corresponding Collaborative measures improvement rates, if appropriate, are detailed below.
Participating HCOs began intervention implementation in September 2023 and continued through February 2025. Throughout this period, they encountered various implementation challenges, including EHR transitions, delays in scheduling EHR modifications, health system mergers, and staffing changes. Their efforts are ongoing, and organizations expect to see continued improvement in 2025 and beyond, supported by sustainability initiatives.
Up-to-Date (UTD) Screening
-
Interventions
-
Population Health sent direct letters to patients due for screening.
-
Streamlined workflows to ensure that Fecal Immunochemical Test (FIT) kits will be readily available at clinics and locations.
-
Partnered with Pathology for bulk order for FIT kits.
-
Identified PCP offices to pilot bulk ordering FIT kits so that it is an open order for eligible patients aged 45 to 75 years old. The open order for FIT will trigger a distribution of a FIT kit when a patient is visiting our diagnostic centers for lab work.
-
Developed script and trained lab staff to discuss the FIT test order with patients when they come for any lab test.
-
-
MEASURE RATES: BASELINE Q2 2023 68.3%; FINAL Q3 2024 72.4%
-
Interventions
-
Adjusted screening rates on provider/clinic dashboards to show increase, as well as provide reports and best practice prompts for clinic staff. Clinics can filter all primary care locations and see rank in comparison with peers. Implemented campaigns and utilized colorectal cancer (CRC) awareness posters during the month of March (Colorectal Cancer Awareness Month).
-
Created monthly report that is sent to all practice managers indicating any stool-based tests that were positive or unable to be processed during the previous month. Clinic staff are tasked with patient outreach to schedule colonoscopy or to have patient recollect the stool sample.
-
Provided education for clinical staff on the closed-loop referral and reviewing in-basket for open orders for any CRC screening. Held conversations with largest GI group on direct scheduling for colonoscopy procedures by clinic staff. This would reduce the volume of missed calls and work for the GI team. Will use the “order up” functionality in Epic.
-
Conducting ongoing education around Social Determinants of Health Questionnaire and ensuring every patient has some type of annual screening for these barriers. Use of FindHelp tool within Epic to connect patients to community resources for transportation or other barriers.
-
-
MEASURE RATES: BASELINE Q2 2023 66.9%; FINAL Q1 2025 75.7%
-
Interventions
-
Standardized internal ordering for colonoscopies across the health system
-
Completion of positive stool test report is available in Epic.
-
Created cultural shift to Fecal Immunochemical Test (FIT) First (or other home testing option) by educating providers in Primary Care regarding home testing options for low-average-risk patients.
-
Utilized Epic Campaigns to automate notification and ordering for patients who are eligible for a Fecal Occult Blood Test (FOBT).
-
Epic Dashboard built for performance transparency and ease of report access for GI to own outreach to patients with a positive stool test.
-
Engaged OB/GYN providers to increase screening rates.
-
-
MEASURE RATES: BASELINE Q2 2023 64.2%; FINAL Q1 2025 72.4%
-
Interventions
-
Worked with marketing department to create social media post(s) targeting the 45-49 age group. Utilized in March 2025 for CRC Awareness Month. Provider featured on local news for CRC Awareness Month.
-
Handout explaining colon cancer screening options added to website. Worked with marketing to configure key search terms to make searchable for patients.
-
Requested IT report to list patients overdue for CRC screening AND have a family history of CRC in first-degree relative. Conducted outreach to those patients.
-
Use the Campaigns module in Epic for automated/continuous outreach to patients who become due for CRC screening.
-
Supported the change in the order for a colonoscopy location to automatically choose the Ambulatory Surgery Center if patient meets criteria. This ensures driving better access and lower costs for patients, the organization, and payors. Staff and provider education presented in meetings promoting ASC site to reduce costs to patients.
-
-
MEASURE RATES: BASELINE Q2 2023 62.1%; FINAL Q1 2025 68.3%
-
Interventions
-
Placed signs from Exact Sciences in clinics indicating starting age and reason for screening.
-
Have FIT screens available in office to hand to patients during the visit.
-
Education was provided for OB/GYN and other non-IM/FM primary care providers regarding screening modalities and recommendations.
-
Explored targeted communications, such as through Emmi, portal messages/letters with patient education, and messaging that patient may be due for screening.
-
Developed clinic workflows to enable staff to prompt patients needing CRC screening and appointing care/quality staff to call patients overdue and close gaps.
-
Partnered with community organizations to increase knowledge via a campaign that uses social media, churches, barber shops, etc.
-
-
MEASURE RATES: BASELINE Q2 2023 64.6%; FINAL Q1 2025 70.2%
Achieving Health Equity
-
Made interventions to increase CRC screening completion within uninsured population. Remain committed to continuing the focus on providing more affordable care and resources for these patients.
-
Plan to maintain a partnership with Cologuard at health fairs and ensure that patient charity opportunities remain a central element of ongoing education throughout the care continuum.
-
Aim to leverage the educational tool developed through the shared decision-making special project to directly impact this patient population, enhancing awareness of alternative screening options to colonoscopies.
-
-
Interventions
-
Implemented video pilot in two separate, but diverse clinics.
-
Translated it into multiple languages.
-
Received feedback from focus groups.
-
Provides a level playing field for everyone with regard to education about CRC screening.
-
-
Sent out MyChart message to those who have an open care gap.
-
-
Interventions for Hispanic patients with limited English proficiency
-
Tracked FIT returns and reached out to remaining patients who did not return FIT kits with local and virtual staff.
-
Investigated potential partnership opportunities with community members.
-
Reevaluated language-appropriate CRC screening education one-sheet to distribute during encounters.
-
-
Interventions
-
Implemented a direct to colonoscopy program in the OB/GYN setting for females 45 and older.
-
Implemented a priority colonoscopy opportunity for female OB/GYN patients with positive Cologuard test and/or family history of polyps.
-
Shared Decision-Making Tool designed and launched at piloted OB/GYN sites.
-
Created and disseminated materials to raise awareness of the need to screen, targeting both OB/GYN physicians and their patients.
-
Partnered with Katz Institute for Women’s Health, held virtual events and discussions, and launched social media campaigns in office to raise awareness.
-
Utilized a patient navigator to facilitate/fast-track patient colonoscopy.
-
- Intervention to improve health equity in “age 45 – 49” and “age 45 – 49 and Race (American Indian, Alaska Native, Native Hawaiian and Other Pacific Islander)”
- Outreach:
- Leveraged care coordinators aligned with individual primary care practices to manage FIT outreach using Epic Reporting Workbench Reports and Health Maintenance. This includes all-staff training refresh, implementing follow-up reminder message at two months, translating communication materials into Spanish, and updates to job aid.
- Identified patients who didn’t read message in EHR (MyChart) and didn’t answer phone, and send physical letter with information about updated guidelines and new screening age, as well as increased prevalence in younger population.
- Partnered with OHSU Health Equity Department and developed Primary Care Equity Strategic Plan.
- Outreach:
Follow-Up Colonoscopy after Abnormal Stool-Based Test
Data key: BASELINE YEAR = Q3 2022, Q4 2022, Q1 2023, and Q2 2023; FINAL YEAR = Q1 2024, Q2 2024, Q3 2024, and Q4 2024. This allows for calculation and comparison of 90-day follow-up colonoscopy completion rates across years.
-
Interventions
-
Created dashboard that identifies positive non-colonoscopy CRC screenings patients. Staff monitor weekly.
-
Nurse practitioner in Gastroenterology Department oversees dashboard and identifies patients who have not followed up with a colonoscopy and also identifies earlier appointment availability for +SBT patients on this dashboard who can be moved to earlier appointment.
-
-
MEASURE RATES: BASELINE YEAR 19.9%; FINAL YEAR 48.1%
-
Interventions
-
Identified positive Cologuard or positive FIT tests.
-
Sent the patient directly to IHS Gastroenterology Screening Procedure Pool.
-
Indicated high priority and note positive Cologuard or positive FIT tests in message.
-
Patient will be contacted within five business days. The procedure date will be scheduled within four to six weeks.
-
MEASURE RATES: BASELINE YEAR 23.9%; FINAL YEAR 38.2%
-
Intervention: Standard Follow-Up Workflow
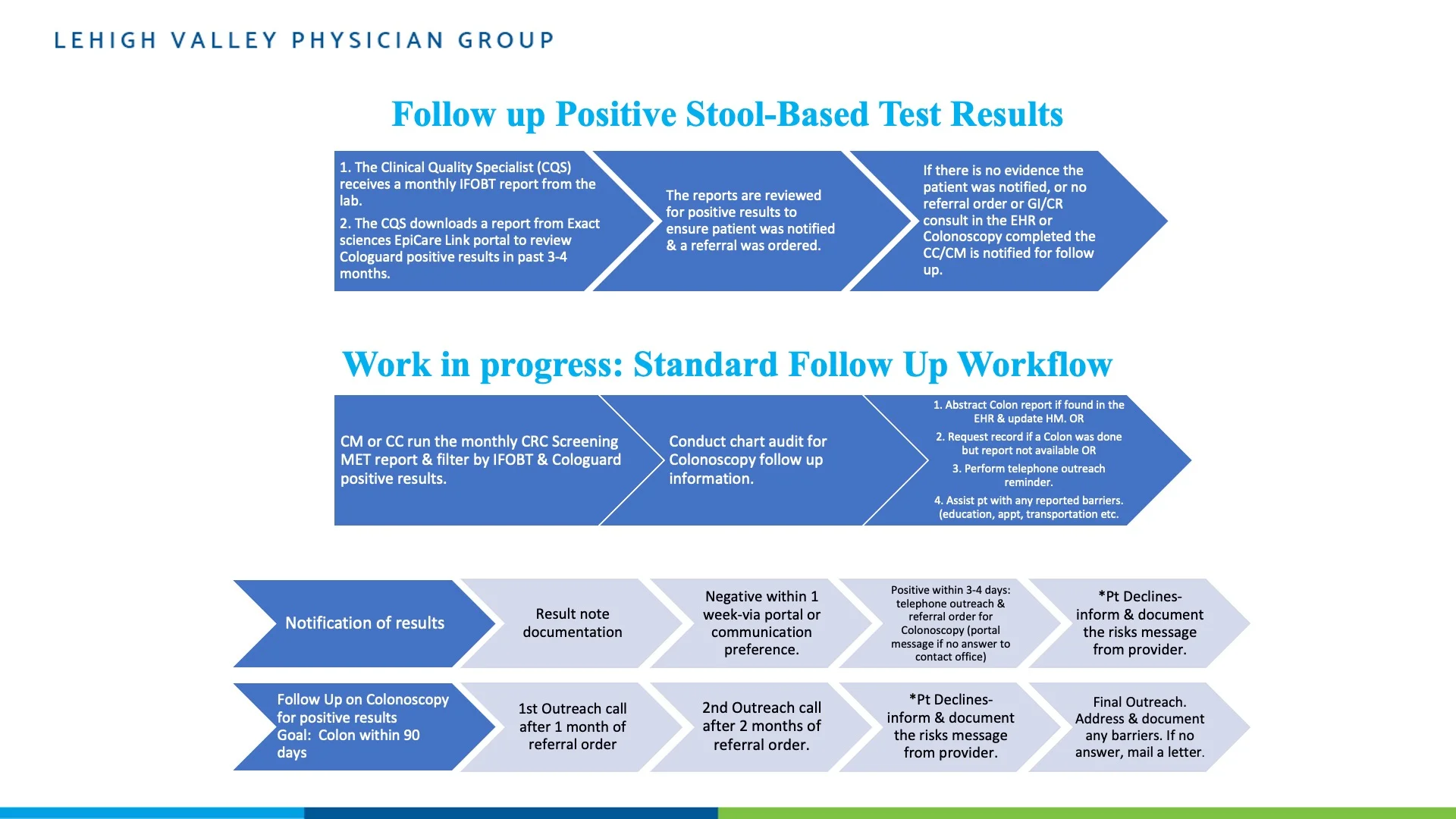
-
Tips
-
Success requires physician champion, clinical leadership, and clinical staff buy-in.
-
Simple workflow and protocol with instructions and SmartPhrases are helpful.
-
Dedicated time for appropriate follow-up and care coordination for positive results is necessary.
-
Standardize a follow-up process for primary care and specialists.
-
Partner with a centralized virtual team for 90-day follow-up after a positive stool-based test.
-
Collaborate with Gastroenterology- and Colorectal-independent physician groups for consistent workflow for access and colonoscopy results.
-
Modify Colonoscopy referral order in Epic to include more information and expand Open Access order.
-
Automate patient and staff reminders: Screening is due, follow-up options, and actions.
-
Create a CRC screening pathway dashboard in Epic with PHI to easily track results, follow-up actions, and patients due for rescreening.
-
-
MEASURE RATES: BASELINE YEAR 30.2%; FINAL YEAR 38.0%
-
-
Interventions
-
Collaboration between primary care and gastroenterology specialist for appropriate expedited referral process using new protocols
-
All non-colonoscopy test results are auto-filed in the EMR.
-
All patients with positive results are contacted using the “As Soon As Possible protocol”; patient is contacted within two days, via telephone (three times) and certified letter.
-
Appointment is scheduled with the internal gastroenterology specialty for colonoscopy.
-
-
-
MEASURE RATES: BASELINE YEAR 39.0%; FINAL YEAR 47.0%
-
Interventions
-
Incorporated CDC tools within the EHR for screening, compliance, and follow up. Created SmartTexts and SmartPhrases to support clinicians.
-
Implemented Exact Sciences Cologuard ordering and results in the EHR.
-
Utilized CRC Screening Navigator with cross-site colonoscopy scheduling access and priority for patients with positive FIT.
-
Gastroenterology providers prioritize positive FIT follow-ups and update colonoscopy HMT frequency.
-
-
MEASURE RATES: BASELINE YEAR 22.9%; FINAL YEAR 38.5%
-
Interventions
-
Integrated with Cologuard’s Epic system to eliminate data entry errors and ensure abnormal results are received timely by the ordering provider.
-
Launched FIT First outreach in MyChart portal.
-
Utilized dashboards to make data readily available, including HEDIS colon cancer screening performance in all ages and percent of patients with colonoscopy follow-up in 90 days after their abnormal stool-based test.
-
Improved data capture throughout the Collaborative helped identify colonoscopies completed outside the system. While this does not reflect an increase in procedures performed, it is essential for accurately measuring improvement efforts.
-
-
MEASURE RATES: BASELINE YEAR 17.2%; FOLLOW-UP YEAR 36.2%
Choice-Based Shared Decision-Making (SDM)
-
Interventions
-
Created a workflow with Cologuard as an option.
-
Initiated widespread use of the American Society for Gastrointestinal Endoscopy (ASGE) shared decision-making flyer in all primary care clinics, as well as in giant, inflatable colon tour. Additionally, offering the Spanish version as a norm to reduce any barriers.
-
Compared performance of provider/clinic in pilot with nonparticipating provider/clinic in closing the gaps of CRC screening.
-
-
Intervention: Introducing New Options in “Colonoscopy First” Environment
-
Three community health clinics were open to creative solutions to increase CRC screening rates, including mailed FIT tests, “Colonoscopy First” approach and collaboration with local programs providing reduced cost/free colonoscopies for patients willing to complete educational courses.
-
Used SDM tool and clinic on-site training to ensure patients understood their screening options and felt comfortable and confident in choosing the screening option that best fits their needs.
-
- Interventions
- Staff education on new shared decision-making tool for patients and conversation with patients. Circulated article for March newsletters to staff for CRC Awareness Month. SDM tool is available in the After Visit Summary.
-
Interventions
-
Materials updated to include the Shared Decision-Making Tool and Cologuard resources.
-
Revised the FIT instruction sheet to increase clarity for patients.
-
Created a new FIT instruction video for patients to understand the importance of CRC screening and how to complete FIT.
-
-
Interventions
-
Co-branded SDM tool and can include clinic-level branding.
-
Created dry erase board, posters, tear-off pads, etc.
-
Tool with identified providers to participate was rolled out to clinics.
-
![]()